Gestational Diabetes - diet, symptoms, dignosis and treatment
What is Gestational Diabetes
Gestational Diabetes - The development of INSULIN RESISTANCE or type 2 DIABETES during PREGNANCY. Gestational diabetes develops between 24 and 28 weeks of pregnancy. Doctors believe the rising levels of hormones the PLACENTA produces at this point in pregnancy interfere with the ability of the woman’s body to properly metabolize INSULIN. Insulin production remains normal. Diabetes that manifests earlier than 24 weeks in pregnancy is nearly always diabetes that was undetected at the start of the pregnancy. Gestational diabetes goes away shortly after delivery, though women who have gestational diabetes have increased risk for developing type 2 diabetes later in life.
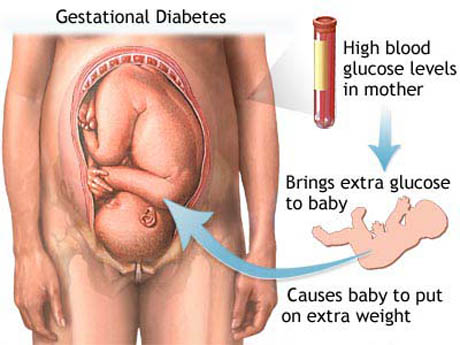
Untreated gestational diabetes poses a health risk primarily for the FETUS. The excessive GLUCOSE (sugar) that circulates in the mother’s BLOOD crosses the placenta. When it reaches the fetus the excessive glucose fuels fetal growth, resulting in fetal size up to 20 percent greater than normal. This growth becomes problematic within the UTERUS as the fetus cannot move as freely. Adequate prenatal movement is important for proper muscular development. A fetus larger than about eight pounds often has difficulty passing through the birth canal. The circumstance of an overly large fetus, called macrosomia, often necessitates birth by CESAREAN SECTION (surgical delivery) to safeguard the health of both baby and mother. As well, the newborn infant may experience HYPOGLYCEMIA (low blood glucose) in the first hours after birth.
Symptoms of Gestational Diabetes and Diagnostic Path
Most often gestational diabetes has few noticeable symptoms. When symptoms do occur they may include frequent URINATION, increased thirst, and increased hunger. Because these are common in pregnancy, however, they are difficult to distinguish as symptoms of diabetes. Routine URINE tests at each prenatal doctor visit screen for the overflow of glucose in the urine, which indicates high blood glucose. Health-care providers routinely test for elevated glucose in the woman’s blood circulation between the 24th and 28th weeks of pregnancy. The most common such test is the three-hour glucose tolerance test. Findings of an elevated blood glucose level at two or more of the four drawings of blood over the course of the test generally establishes the diagnosis of gestational diabetes.
Gestational Diabetes Treatment Options and Outlook
Many women are able to manage gestational diabetes through nutritional EATING HABITS and daily exercise. Women for whom lifestyle measures do not maintain stable blood glucose levels typically require insulin injections through the remainder of pregnancy. The safety of oral antidiabetes medications in pregnancy remains undetermined, though some doctors offer this treatment. Diligent management of blood glucose levels helps maintain normal growth and weight of the fetus.
In nearly all women gestational diabetes goes away within a week of delivery and for a third of women diabetes is never again a health concern. However, in some women who have high risk for diabetes in the first place gestational diabetes may persist to become conventional diabetes. One in five women who has gestational diabetes will develop conventional diabetes within five years of her baby’s birth, and about two thirds of women will develop the condition later in life.
Gestational Diabetes - Risk Factors and Preventive Measures
Any pregnant woman can develop gestational diabetes. Factors that increase the risk for gestational diabetes include
- gestational diabetes in a previous pregnancy
- obesity
- African American or Hispanic heritage
- age 25 or older
Because gestational diabetes results from the effects in the woman’s body of hormones the placenta produces, there are no certain measures to prevent its development. Lifestyle measures to maintain nutritious eating habits, daily exercise, and healthy weight help the body use glucose and insulin as efficiently as possible.
See also ECLAMPSIA; LIFESTYLE AND HEALTH; PREECLAMPSIA; WEIGHT LOSS AND WEIGHT MANAGEMENT.