Congenital Heart Disease
Congenital Heart Disease - HEART conditions, including structural anomalies of the heart, that are present from birth. Some forms of congenital heart disease are mild to moderate and require minimal or one-time intervention to correct. Congenital heart malformations are among the most common BIRTH DEFECTS in the United States. Though still the leading cause of infant death due to birth defects, congenital heart malformations no longer mean certain death. Beginning in the 1950s pediatric cardiology pioneers Alfred Blalock (1899–1964), Helen Taussig (1898–1986), and Vivien Thomas (1910–1985) established many of the operations and surgical techniques that remain in use today to create functional BLOOD flow through malformed hearts. Advances in CARDIOPULMONARY BYPASS and refinements in surgical techniques have made relatively normal lives possible for more than a million children with heart defects born since 1970.
Structural deformities that affect the heart’s ability to circulate oxygenated blood result in inadequate oxygen reaching the body’s tissues and cause CYANOSIS, a bluish tint to the lips, nail beds, mucous membranes, and SKIN. Doctors collectively refer to these conditions as cyanotic heart disease (sometimes called blue baby syndrome). These conditions are nearly always apparent within 48 hours of birth and typically require fairly immediate intervention (usually surgery). Other forms of congenital heart disease, such as LONG QT SYNDROME (LQTS) and hypertrophic CARDIOMYOPATHY, may not manifest until late childhood or adulthood.
Heart defects may occur in isolation or in combination with GENETIC DISORDERS such as DOWN SYNDROME (trisomy 21) and MARFAN SYNDROME. Heart abnormalities often occur in association with abnormalities of the skeletal, urinary, and gastrointestinal systems, forming a collection that doctors refer to by the acronym VACTERL: vertebral, anorectal, cardiac, tracheoesophageal, renal, and limb. About 50 percent of infants born with one congenital anomaly among this grouping have at least one other. Researchers believe about 10 percent of congenital heart malformations result from GENE MUTATION or CHROMOSOME abnormalities.
Common forms of congenital heart disease
The most common and most easily treatable congenital heart malformations are patent ductus arteriosus (PDA) and septal defects. The ductus arteriosus is an opening between the AORTA and the pulmonary ARTERY in the FETUS that allows fetal circulation to bypass the nonfunctioning LUNGS (the fetus draws oxygen from the mother’s blood supply). At birth a sequence of events takes place, initiated with the pressure changes that occur with the infant’s first breath, that cause the ductus arteriosus to close. In some infants, especially those born prematurely, the closure does not take place and the ductus arteriosus remains patent, or open. PDA allows oxygenated and deoxygenated blood to mix in the pulmonary artery, with the result that the blood the aorta sends to the body carries only partial oxygenation.
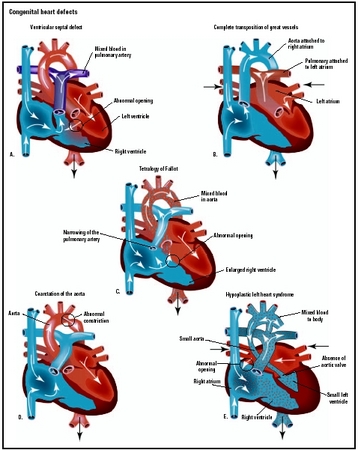
In a septal defect there is an abnormal opening in the septum, or wall, separating the heart’s chambers. A septal defect allows blood to move directly between the involved chambers, which disturbs the flow of blood and can result in blood turbulence and pooling as well as reduced OXYGENATION. The most common presentation is atrial septal defect (ASD), in which the opening is between the right and left atria. The opening may be the result of incomplete closure of the foramen ovale, a natural opening between the atria in the fetus that normally closes within 48 hours of birth. ASD may also occur as a malformation of the atrial septum. A ventricular septal defect (VSD) is a malformation of the ventricular septum and results in an opening between the right and left ventricles. A VSD allows oxygenated and deoxygenated blood to mingle, reducing the oxygen content of the blood the left ventricle pumps out to the body.
Atrioventricular (AV) canal defect is a more extensive malformation of the septum in which the atrial septum, the ventricular septum, or the entire septum is missing. The heart becomes essentially a single large chamber with oxygenated and deoxygenated blood mixing freely. Blood going to the body carries insufficient oxygen, and blood going to the lungs is under much higher pressure than the lungs can accommodate. AV canal defect requires surgical repair within the first few months of the infant’s life. Though AV canal defect can occur as an isolated malformation it most often occurs in conjunction with Down syndrome, affecting about 25 percent of Down syndrome infants.
Other common congenital heart defects include coarctation of the AORTA (narrowing and irregularities) and malformations of the heart valves such as AORTIC STENOSIS, bicuspid aortic valve, tricuspid atresia, and pulmonary atresia.
Grave malformations of the heart
A number of heart malformations are rare, complex, and lifethreatening. Their defects are severe and include alterations of the heart’s structure that cannot sustain life. They require immediate surgery for survival and usually follow-up operations for further reconstruction. In some cases the only viable longterm treatment is HEART TRANSPLANTATION. The most frequently occurring of these grave malformations are
- Tetralogy of Fallot, which is a complex of four structural anomalies: VSD, pulmonary artery and valve malformation, aortic displacement (the aorta arises between the ventricles rather than solely from the left ventricle), and hypertrophic left ventricle (thickening of the left ventricle’s wall).
- Transposition of the great arteries (TGA), in which the aorta and the pulmonary artery are switched. The aorta arises from the right ventricle instead of the left, carrying the deoxygenated blood from the right ventricle out to the body. The pulmonary artery arises from the left ventricle instead of the right, taking oxygenated blood back to the lungs from the left ventricle.
- Hypoplastic (or hypotrophic) left heart syndrome (HLHS), in which the left ventricle or the entire left heart fails to develop, resulting in essentially a two-chamber heart. The aorta is usually small or deformed. Blood in the heart is a mix of oxygenated and deoxygenated, and the right ventricle pumps to both the lungs and the body.
- Persistent truncus arteriosus, which is a combination of VSD and deformities of the PULMONARY ARTERIES and aorta that disrupts the heart’s ability to pump oxygenated blood to the body.
- Anomalous pulmonary venous return, in which the PULMONARY VEINS attach to the right atrium instead of the left atrium, returning oxygenated blood to the same chamber that pumps deoxygenated blood to the lungs. This malformation typically occurs in combination with ASD, so the flow of blood between the atria moves some oxygenated blood into the left atrium and subsequently the left ventricle.
Often, ULTRASOUND during PREGNANCY reveals these significant heart deformities, allowing the neonatal team to be prepared for them at the infant’s birth. In many situations initial treatment includes administering PROSTAGLANDINS to maintain a patent ductus arteriosus, which allows some oxygenated blood into the body’s circulation.
Congenital heart disease in adults
Some forms of congenital heart disease first manifest in adulthood, such as hypertrophic cardiomyopathy and LQTS. Other forms of heart disease in adults may have congenital origins, such as the ARRHYTHMIA disorder WOLFF-PARKINSON-WHITE SYNDROME and some VALVULAR HEART DISEASE. Cardiologists believe that most situations of SUDDEN CARDIAC DEATH reflect undetected congenital heart anomalies, either structural or functional (arrhythmias). With congenital heart disease, whether undetected or previously treated, comes increased risk for ENDOCARDITIS (especially with valve malformations), arrhythmias, and clot formation leading to HEART ATTACK, STROKE, or PULMONARY EMBOLISM.
A growing number of adults had corrective surgery for congenital heart disease as infants or children. Cardiologists do not yet know the long-term effects of these operations or what precautions are necessary to protect cardiovascular health later in life. The generation born in the 1970s was the first to have these options available. As this generation comes into middle age, cardiologists will learn much about how repaired hearts accommodate the routine cardiovascular stresses of life and whether they are more susceptible to acquired forms of heart disease such as CORONARY ARTERY DISEASE (CAD) and HEART FAILURE. At present, the longest survival of infant heart transplantation is 15 years and of adolescent heart transplantation is 16 years. Rejection of the donor heart remains a significant concern, and most cardiologists expect retransplantation will become necessary for most people who receive heart transplants in infancy or childhood.
Symptoms and Diagnostic Path
The most common symptoms of congenital heart disease, notably malformations of the heart, in newborns is cyanosis and difficulty BREATHING. Congenital heart disease not immediately apparent at birth may manifest later in childhood with symptoms such as fainting with physical exertion, shortness of breath with mild activity, slowed growth, rapid heartbeat and respirations, and frequent upper respiratory infections. Young children experiencing shortness of breath often squat, which makes it easier for them to breathe.
Congenital heart disease that manifests in adulthood, such as ASD and hypertrophic cardiomyopathy, often produces symptoms such as PALPITATIONS, shortness of breath, and pulmonary or generalized EDEMA if the heart’s pumping capability becomes ineffective (heart failure). The diagnostic path may include ELECTROCARDIOGRAM (ECG), ECHOCARDIOGRAM, and COMPUTED TOMOGRAPHY (CT) SCAN or MAGNETIC RESONANCE IMAGING (MRI), and CARDIAC CATHETERIZATION.
Treatment Options and Outlook
Minor congenital heart defects may require only watchful waiting. Most ASDs close within 2 years of birth and VSDs by age 7. Septal defects that persist and cause symptoms may require surgery, often via cardiac catheterization to patch the defect. Surgery is the most viable treatment option for most serious malformations of the heart. Surgery may be corrective, in which the OPERATION returns the heart to normal structure and function, or palliative, in which the operation relieves symptoms though does not restore normal structure and function. Surgery may be isolated, in which a single operation corrects the defect, or staged, in which the surgeon performs several sequential operations over a period of time. Some congenital heart malformations require surgery within days of birth, and others within months to 2 or 3 years.
When doctors detect significant congenital defects before or shortly after birth, they often administer prostaglandins to maintain a patent ductus arteriosus. Though in ordinary circumstances a PDA would be a heart defect, in the presence of congenital heart defects PDA allows continued though limited circulation of oxygenated blood to buy time until the infant is stable enough for surgery. In some circumstances the neonatal cardiologist may perform a balloon septostomy to surgically create an ASD, which further allows a mixture of oxygenated and deoxygenated blood to flow from the heart to the body.
Risk Factors and Preventive Measures
Genetic factors are emerging as the likely causes, or at least precipitating circumstances, for many forms of congenital heart disease. There are clear genetic links for conditions such as hypertrophic cardiomyopathy and LQTS, for example, as well as known correlations between specific heart malformations and genetic disorders such as Down syndrome and TURNER’S SYNDROME. As well, the VACTERL constellation of birth defects speaks to genetic underpinnings. Prevention for these kinds of heart problems remains uncertain, though future treatment is likely to include GENE THERAPY.
Some congenital heart malformations occur as the result of maternal infections such as RUBELLA (German MEASLES). Heart defects in infants are more likely to occur with mothers who have DIABETES. Numerous medications, both prescription and over-the-counter, as well as ALCOHOL consumption also cause specific kinds of birth defects. Women who are pregnant or planning to become pregnant should discuss with their doctors any routine medications they take. Many ANTISEIZURE MEDICATIONS and ANTIPSYCHOTIC MEDICATIONS are especially damaging to the developing fetus.
Despite advances in gene technology and knowledge of the body, much congenital heart disease is idiopathic—that is, doctors do not know why it occurs. Studies suggest that folic acid supplementation, which doctors already recommend to reduce the risk for NEURAL TUBE DEFECTS, also reduces the risk for malformations of the heart. Like the neurologic system, the cardiovascular system evolves early in fetal development so most malformations occur in the first weeks of pregnancy. Doctors can detect many heart abnormalities before birth, allowing parents and doctors to make appropriate treatment decisions.
See also CARDIOVASCULAR DISEASE PREVENTION; INFECTION; KAWASAKI DISEASE; SURGERY BENEFIT AND RISK ASSESSMENT; VEIN.